
Hemorrhoidectomy: The surgical removal of excess tissue that causes bleeding and pain.most effective and complete way to treat severe or recurring piles.
Hemorrhoid Stapling: A procedure that blocks blood flow to the hemorrhoidal tissue and staples prolapsed hemorrhoids back into place. It usually involves less pain than a traditional hemorrhoidectomy.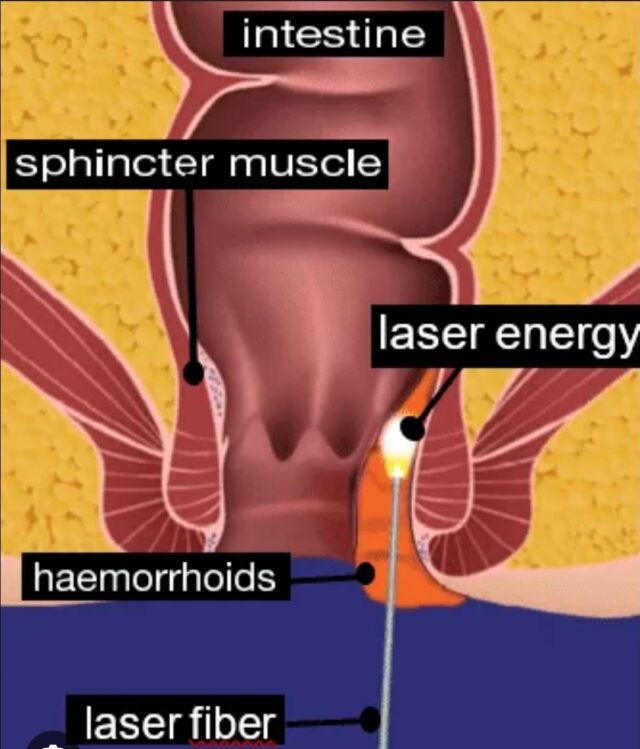
Latest Surgical Treatments for Hemorrhoids: Focus on Laser and Specialized Approaches
Recent advancements in hemorrhoid treatment emphasize minimally invasive techniques that reduce pain, recovery time, and complications compared to traditional surgery. As of the latest research (up to 2023-2024), key surgical options include excisional hemorrhoidectomy (EH), stapled hemorrhoidopexy (SH), Doppler-guided hemorrhoidal artery ligation (DG-HAL), and emerging procedures like laser hemorrhoidoplasty (LH) and hemorrhoidal artery embolization (HAE). Laser treatments are among the most researched energy-based therapies, showing shorter surgery times, less bleeding, and faster return to activities.
FAQ
Is Laser Treatment Effective, and What Types Exist?
Yes, laser treatment is a highly effective, modern surgical option, particularly laser hemorrhoidoplasty (LH), which uses a diode laser to coagulate and shrink hemorrhoid tissue. It offers significant benefits like reduced intraoperative bleeding (by about 20 mL on average), shorter operative time (12-15 minutes less), lower postoperative bleeding risk, and quicker recovery (up to 12 days faster return to daily activities), with no difference in 12-month recurrence rates compared to traditional methods.
Laser treatments are versatile but tailored to hemorrhoid severity and type:
Types of Laser Treatments by Hemorrhoid Grade/Type
Hemorrhoid Type/Grade / Recommended Laser Approach
Grade I-II (Internal, mild bleeding/prolapse) Laser coagulation or ablation Minimally invasive; targets small vessels with infrared or diode lasers for precise shrinkage. Often combined with office procedures like rubber band ligation (RBL).
Grade III (Prolapsing, manual reduction needed) Laser hemorrhoidoplasty (LH) or laser surgery | 1470 nm diode laser probe inserted via stab incision to coagulate tissue between hemorrhoid and anal sphincter. Ideal for multiple/recurrent cases; less pain than EH.
Grade IV (Severe prolapse/irreducible) LH combined with excision or stapling | For large prolapses; laser reduces tissue volume before stapled hemorrhoidopexy (SH). Not standalone for very large cases—may need traditional surgery.
External Hemorrhoids Laser excision or ablation Surgical laser removal for thrombosed cases; quick healing (2-3 weeks), less postoperative pain.
Mixed (Internal + External) Comprehensive LH or laser surgery | Addresses both components; effective for symptom relief in complex cases.
Note on LH specifics: The procedure involves a thin 1.8 mm probe delivering energy to induce fibrosis and shrink tissue, promoting adhesion. Standardization of energy delivery and anesthesia (local to general) is still evolving, with ongoing research needed for cost-effectiveness.
Other Cutting-Edge Surgical Treatments
Beyond lasers, recent innovations focus on vessel-targeted and hybrid approaches:
Hemorrhoidal Artery Embolization (HAE): A non-surgical interventional radiology procedure (pinhole access via wrist/groin). Blocks blood flow to hemorrhoids, shrinking them gradually. Effective for bleeding (65-85% resolution), safe for high-risk patients, with fewer complications than surgery (no swelling, fissures, or incontinence reported in trials). Repeatable if needed.
Stapled Hemorrhoidopexy (SH) Evolutions: Partial “C-shaped” stapling (2021 technique) for grade III-IV to avoid stenosis/fistulas. Often combined with DG-HAL for better outcomes in mixed hemorrhoids.[1]
DG-HAL + Rectoanal Repair (HAL-RAR) Doppler-guided ligation of arteries causing fibrosis and fixation. Lower pain than EH but higher recurrence; enhanced when added to SH or minimal mucosal hemorrhoidectomy (MMH).
Hybrid/Mixed Techniques: For severe cases, combine HAL with EH/SH to minimize pain, bleeding, and prolapse recurrence (2023 studies).
– Endoscopic Options: Flexible endoscopy with sclerotherapy or coagulation for precise, low-risk treatment.
Traditional EH remains gold standard for grade III-IV but carries higher risks (pain, stenosis, incontinence). Always consult a specialist—procedures like LH or HAE suit outpatient settings with rapid recovery.
Disclaimer: While this article provides educational information, it is always highly recommended to consult a gastroenterologist if you experience bleeding, severe pain, or if symptoms do not improve with home treatments.